Influence of higher valve gradient on long-term outcome after aortic valve repair
Abstract
Objective: To evaluate the effect of higher post-operative valve gradient on freedom from valve reintervention and death in patients undergoing aortic valve repair (AVr).
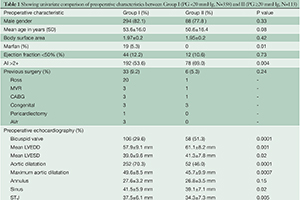
Methods: Patients who underwent AVr between March 1996 and June 2010 were divided into 2 groups: I: peak gradient (PG) <20 mmHg (n=358) and II: PG ≥20 mmHg (n=113). Age (53.6±16.0 vs. 50.6±16.4 years; P=0.08), impaired LV (n=44, 12.2% vs. n=12, 10.6%: P=0.73) as well as the body surface area (1.97 vs. 1.95 m2; P=0.4) were similar. Pre-operative AI >2+ was greater in Group II compared to Group I (n=78, 69.0% vs. n=192, 53.6 %; P=0.004). Patients in Group II had higher proportion of bicuspid valves (BV) (n=58, 51.3% vs. n=106, 29.6%; P=0.0001) and restrictive valves (n=34, 30.0% vs. n=52, 14.5%; P=0.0001) while Marfan patients were seen only in Group I (n=19; P=0.010). Mean follow-up for Group I and Group II was 123.1±89.7 and 147.1±108.0 months, respectively.
Results: In-hospital mortality was n=2 (0.5%) for Group I and none for Group II (P=1.0). Valve-sparing was higher in Group I (P=0.0001) but sub-commissural annuloplasty was similar (P=0.15). Shaving and/ or decalcification was performed more in Group II (n=68, 60.1% vs. n=117, 32.6%; P=0.0001). Logistic regression analysis identified calcified, restrictive and bicuspid valves as independent predictors of PG ≥ 20 mmHg (P=0.04 for each). Predictors of re-operation were increased end-diastolic diameter (P=0.03) and younger age (P=0.007), but not PG ≥20 mmHg (P=0.98) (based on logistic regression). Overall 10-year cardiac survival and freedom from AV re-intervention was 82.3±4.6% vs. 89.5±4.2% (P=0.53) and 89.1±3.0% vs. 76.8±8.4% (P=0.02), in Group I and II, respectively (based on Kaplan-Meier analysis). Sub-group analysis showed that Group II patients requiring re-intervention (n=10) were younger (41.8±13.1 vs. 51.0±16.0 years; P=0.08) with similar proportion of bicuspid valves (n=6; 60%; P=0.74). The main reason for AV re-operation was aortic insufficiency (n=7) and AI + stenosis (n=3).
Conclusions: Higher gradient after AVr is associated with a reduced freedom from AV re-intervention, especially in younger patients.
Cover