Extended thoracic lymph node dissection in robotic-assisted minimal invasive esophagectomy (RAMIE) for patients with superior mediastinal lymph node metastasis
Abstract
Background: Robot-assisted surgery may have a role in improving oncological outcomes in esophagectomy. Especially in the anatomical areas in the chest that are more difficult to reach in open surgery (including the superior mediastinum). The dexterity of the robotic instruments aid in performing a more extensive nodal dissection and the precision and detailed vision of the robotic system potentially improves staging, oncological outcomes and reduces complications (i.e., recurrent nerve palsy). In this article, we describe our experience and clinical outcomes in patients treated by robot assisted minimal invasive esophagectomy (RAMIE) in cN+ esophageal cancer patients with positive nodes localized in the superior mediastinum.
Methods: From May 2007–2018, all patients who had involved nodes by either fluor-18-deoxyglucose positron-emission-tomography-computed tomography (FDG-PET-CT) or endoscopic ultrasound (EUS) + fine needle aspiration (FNA) localized in the superior mediastinum (above level Th4/sternal angle) were identified. Patient characteristics, perioperative data, postoperative clinical outcomes/complications and overall survival were prospectively recorded and retrospectively evaluated.
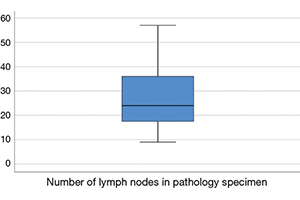
Results: Forty patients (48% adenocarcinoma) met our inclusion criteria. All patients underwent a three-stage procedure with cervical anastomosis and 90% of the patients underwent neoadjuvant chemoradiotherapy. Mortality occurred in three patients (7.5%), of which two were caused by severe acute respiratory distress syndrome (ARDS). The most frequent complications were pneumonia (25%), chylothorax (20%), anastomotic leakage (17.5%) and vocal cord paralysis (17.5%) which was grade 1 in 72% of the patients. Radicality rate (R0 resection) was 98% and the average lymph node yield was 24 (range, 9–57). Median overall and disease-free survival was 26 and 17 months, respectively.
Conclusions: RAMIE for esophageal cancer patients with node positive disease in the superior mediastinum is associated with increased mortality/morbidity. Oncological outcome showed excellent lymph node yield, R0 rate and survival was equal compared to patients with lower mediastinal node positive disease.
Cover