Renal protective effect of the aortic balloon occlusion technique in total arch replacement with frozen elephant trunk
Abstract
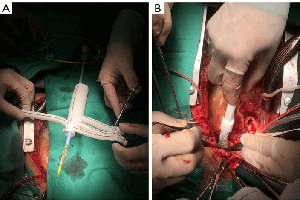
Background: Organ dysfunction caused by hypothermic circulatory arrest continues to concern surgeons. The aortic balloon occlusion (ABO) technique can significantly shorten the circulatory arrest time in total arch replacement with frozen elephant trunk (TAR with FET). This study aims to analyze the renal protective effect of the ABO technique and to analyze the predictors of acute kidney injury (AKI) and continuous renal replacement therapy (CRRT) after TAR with FET.
Methods: Between August 2017 and September 2018, 247 patients who underwent TAR with FET were divided into ABO and moderate hypothermic circulatory arrest (MHCA) groups. The primary endpoint was postoperative AKI defined by the Kidney Disease Improving Global Outcomes (KDIGO) criteria. Multivariable logistic analysis was used to identify the predictors of AKI and CRRT after TAR with FET.
Results: With the application of the ABO technique, the circulatory arrest time was significantly shortened (ABO 4, IQR: 3–6 vs. MHCA 18, IQR: 16–20, P<0.001). Meanwhile, surgeons safely set the lowest nasopharyngeal temperature at a higher grade (ABO 28.1, IQR: 27.4–28.5 vs. MHCA 24.7, IQR: 24.1–25.1, P<0.001). The peak serum creatinine (SCr) values within 48 hours after the surgery was lower in the ABO group than in the MHCA group (ABO 124, IQR: 97–173 vs. MHCA 146, IQR: 108–221, P=0.008). The distribution of AKI grade according to the KDIGO criteria differed between the two groups (P=0.04): more patients in the ABO group were free from AKI (Grade 0) than patients in the MHCA group (33% vs. 23.1%), and the proportion of patients with high-grade AKI (Grades 2 and 3) in the ABO group was lower than that in the MHCA group (21% vs. 32%). The ABO technique was associated with reduced potential for AKI, but was not protective for CRRT.
Conclusions: The ABO technique significantly shortened the circulatory arrest time and safely elevated temperature, and provided better renal protection in patients undergoing TAR with FET. The ABO technique did not reverse the need for CRRT, nor did it reduce mortality or major adverse events.
Cover