Total aortic arch replacement: current approach using the trifurcated graft technique
Abstract
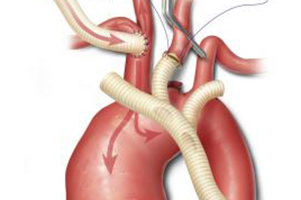
Since the pioneering work of DeBakey, Cooley, and colleagues more than 50 years ago, surgical treatment of aneurysms involving the transverse aortic arch has been associated with substantial morbidity and mortality. Over the past 15 years, techniques for replacing the diseased aortic arch have evolved substantially. Previously, our approach to these operations involved femoral cannulation, profound-to-deep hypothermic circulatory arrest and retrograde cerebral perfusion, and the island technique for reattaching the brachiocephalic vessels. In contrast, we currently use innominate artery cannulation, deep-to-moderate hypothermic circulatory arrest with antegrade cerebral perfusion, bilateral cerebral monitoring with near-infrared spectroscopy, and the trifurcated graft (Y-graft) technique for reattaching the arch branches. Cannulating the innominate artery to provide an inflow site for cardiopulmonary bypass has facilitated the use of antegrade cerebral perfusion as a cerebral protection strategy; the left common carotid artery is additionally perfused to provide bilateral cerebral perfusion. Despite having a systemic circulatory arrest time that often exceeds 60 minutes, these improved perfusion strategies make it possible to consistently avoid cerebral circulatory arrest all together. A moderate temperature target of between 18°C and 23°C is now used; this appears to reduce the risk of hypothermic coagulopathy and improve hemostasis. Y-graft techniques, such as the trifurcated graft approach, have the advantages of eliminating residual aortic arch tissue and being easily tailored to the needs of the individual patient. This report describes total aortic arch replacement in patients with aneurysms that are confined to the ascending aorta and transverse aortic arch.
Cover