Overview of adult congenital heart transplants
Abstract
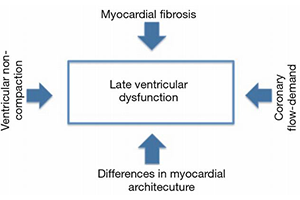
Transplantation for adult patients with congenital heart disease (ACHD) is a growing clinical endeavor in the transplant community. Understanding the results and defining potential high-risk patient subsets will allow optimization of patient outcomes. This review summarizes the scope of ACHD transplantation, the mechanisms of late ventricular dysfunction, the ACHD population at risk of developing heart failure, the indications and potential contraindications for transplant, surgical considerations, and post-transplant outcomes. The findings reveal that 3.3% of adult heart transplants occur in ACHD patients. The potential mechanisms for the development of late ventricular dysfunction include a morphologic systemic right ventricle, altered coronary perfusion, and ventricular noncompaction. The indications for transplant in ACHD patients include systemic ventricular failure refractory medical therapy, Fontan patients failing from chronic passive pulmonary circulation, and progressive cyanosis leading to functional decline. Transplantation in ACHD patients can be quite complex and may require extensive reconstruction of the branch pulmonary arteries, systemic veins, or the aorta. Vasoplegia, bleeding, and graft right ventricular dysfunction can complicate the immediate post-transplant period. The post-transplant operative mortality ranges between 14% and 39%. The majority of early mortality occurs in ACHD patients with univentricular congenital heart disease. However, there has been improvement in operative survival in more contemporary studies. In conclusion, the experience with cardiac transplantation for ACHD patients with end-stage heart failure is growing, and high-risk patient subsets have been defined. Significant strides have been made in developing evidence-based guidelines of indications for transplant, and the intraoperative management of complex reconstruction has evolved. With proper patient selection, more aggressive use of mechanical circulatory support, and earlier referral of patients with failing Fontan physiology, outcomes should continue to improve.
Cover