Systematic review of robotic minimally invasive mitral valve surgery
Abstract
Background: Robotic telemanipulators have evolved to assist the challenges of minimally invasive mitral valve surgery (MVS). A systematic review was performed to provide a synopsis of the literature, focusing on clinical outcomes and cost-effectiveness.
Method: Structured searches of MEDLINE, Embase, and Cochrane databases were performed in August 2013. All original studies except case-reports were included in qualitative review. Studies with ≥50 patients were presented quantitatively.
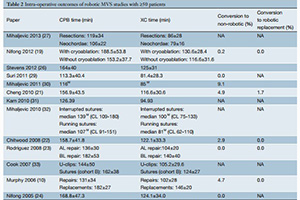
Results: After applying inclusion and exclusion criteria to the search results, 27 studies were included in qualitative review, 16 of which had ≥50 patients. All studies were observational in nature, and thus the quality of evidence was rated low to medium. Patients generally had good left ventricular performance, were relatively asymptomatic, and mean patient age ranged from 52.6-58.4 years. Rates of intraoperative outcomes ranged from: 0.0-9.1% for conversion to non-robotic surgery, 106±22 to 188.5±53.8 min for cardiopulmonary bypass (CPB) time and 79±16 to 140±40 min for cross-clamp (XC) time. Rates of short-term postoperative outcomes ranged from: 0.0-3.0% for mortality, 0.0-3.2% for myocardial infarction (MI), 0.0-3.0% for permanent stroke, 1.6-15% for pleural effusion, 0.0-5.0% for reoperations for bleeding, 0.0-0.3% for infection, and 1.1-6% for prolonged ventilation (>48 hours), 1.5-5.4% for early repair failure, 12.3±6.7 to 36.6±24.7 hours for intensive care length of stay, 3.1±0.3 to 6.3±3.9 days for hospital length of stay (HLOS) and 81.7-97.6% had no or trivial mitral regurgitation (MR) before discharge.
Conclusions: All subtypes of mitral valve prolapse are repairable with robotic techniques. CPB and XC times are long, and novel techniques such as the Cor-Knot, Nitinol clips or running sutures may reduce the time required. The overall rates of early postoperative mortality and morbidity are low. Improvements in postoperative quality of life (QoL) and expeditious return to work offset the increase in equipment and intraoperative cost. Evidence for long-term outcomes is as yet limited.
Cover