Minimally invasive staged segmental artery coil embolization (MIS2ACE) for spinal cord protection
Abstract
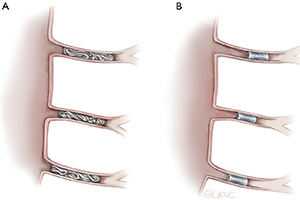
Minimally invasive staged segmental artery coil embolization (MIS2ACE) is an emerging technology for priming of the paraspinous collateral network prior to open or endovascular thoracoabdominal aortic aneurysm (TAAA) repair. Its safety and efficacy have been previously proven in various experimental settings and confirmed in numerous multicentric pilot studies for open and endovascular repair. MIS2ACE is safe and has the potential to decisively reduce the risk of postoperative paraplegia, the most devastating complication of open and endovascular TAAA repair, still affecting up to 20% of patients. Up to now, MIS2ACE has been clinically implemented with excellent results, and is currently being investigated in the international, multicenter, randomized controlled trial PAPAartis, funded by the German Research foundation, and the European Union. MIS2ACE can be performed under local anesthesia, enabling continuous monitoring of neurological function, and in case of clinical signs of imminent ischemia, preemptive interruption of the procedure. A thorough evaluation of preoperative computed tomography (CT) imaging for identification of open and accessible segmental arteries (SAs) is critical. Segmental artery occlusion can be achieved with either micro coils, or vascular plugs. A maximum number of seven SAs is currently recommended to be occluded in the same session, and a minimum interval of 5 days should be awaited between either two MIS2ACE sessions or between MIS2ACE and the final repair. Adjuvant side-effects of MIS2ACE are the reduction in segmental back-bleeding during open repair leading to harmful steal phenomenon and the reduction of the incidence of type II endoleaks in endovascular repair. Current contraindications for MIS2ACE are emergency cases, hostile anatomy, and a shaggy aorta. Other neuroprotective adjuncts such as cerebrospinal fluid (CSF) drainage, permissive hypertension, motor-evoked potentials (MEP)/somato-sensory evoked potentials (SSEP) and monitoring of paraspinous muscle oxygenation by near-infrared spectroscopy should also be applied independent of prior MIS2ACE procedure.
Cover