Thoracoabdominal aortic aneurysm in women: many questions remain regarding their poor outcome
Abstract
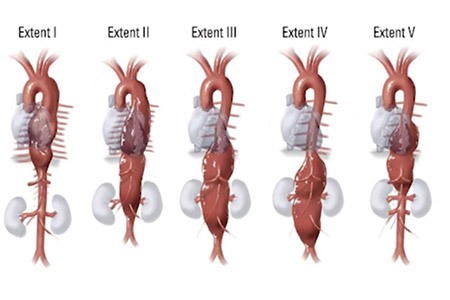
Thoracoabdominal aortic aneurysms (TAAAs) affect approximately 5.9/100,000 persons per year, with a male:female ratio of approximately 1.5–1.7:1. Data exploring sex-related variations in epidemiology and clinical presentation are scarce, as women are normally under-represented in clinical trials. As female hormones and their receptors greatly impact the functions of the vascular cells and aneurysm etiology and extent, the age at surgery and comorbidities also differ between men and women. Additionally, female patients have smaller anatomic structures, including visceral/infrarenal aorta and iliac arteries, than most men. Thus, aneurysms of a certain diameter can represent more advanced disease in women comparatively, than the same-sized aneurysms in males, and be the cause of delayed and often emergent treatment. Adjusting the aortic diameter threshold is recommended for surgery using aortic size index (ASI) [aortic diameter in cm/body surface area (BSA) in m2] or aortic height index (AHI) (aortic diameter in cm/patient height in m) indices in patients who are significantly shorter or taller than average, but no specific sex-related size criteria have been indicated so far for TAAA. Data about TAAA outcomes are conflicting, but female sex has been demonstrated to be an independent risk factor for increased major postoperative complications (i.e., bleeding, acute limb ischemia, renal failure, bowel ischemia, spinal cord ischemia) with longer hospital and intensive unit care stay and in-hospital and 30-day mortality following endovascular treatment and increased long-term mortality following open repair. Despite this evidence, sex does not influence TAAA management strategies and currently the allocation to open or endovascular repair is based on anatomy and clinical setting. In light of these disadvantaged outcomes, further efforts are needed to better understand the sex-related differences in the TAAA diagnosis and management in order to allow prompt and appropriate treatment of female patients.
Cover